
PDF Download
Abstract
The current administration’s incentive for EMR adoption has generated a lot of excitement in the healthcare industry. By 2015, all physician practices and hospitals are required to have implemented an EMR system. Wide adoption of EMR would address many of the problems bedeviling the U.S. healthcare system through interoperability and easy access to current patient records. This would make the healthcare system more efficient, improve quality of care and reduce health care costs by minimizing medical errors, redundant tests and redundant procedures. The Congressional Budget Office (CBO) projected $12 billion saving from health IT over 10 years. However, physicians in small health care delivery environment argue that costs of EMR adoption and maintenance will exceed the benefits. This is because the cost of hardware, software, maintenance, and digitizing existing records can be prohibitive. Besides, most of the current EMR systems are largely focused on recreating the current paper-based system. There is no thought given to how patient data can help physicians make better care decisions. An ideal EMR system will combine documentation with enhanced usability and superior decision support system.
The use of Electronic Medical Records (EMRs) in the U.S. started in the 1960s in a few health care providing institutions. In the 1970s and 1980s, a number of hospitals and clinics across the U.S. adopted the use of limited EMR technology.1 In the early 1990s, heeding recommendations from the Institute of Medicine (IOM) landmark study, the U.S. government set an ambitious goal for all physicians to computerize patient records by the year 2000.2 Due to patients’ privacy issues, less streamlined and often conflicting software technologies, and multiple other barriers in EMR technology adoption, this goal could not be achieved. The adoption of EMR technology started to gather some momentum since 2004 when President George Bush outlined detailed plan to ensure access of electronic health records by all Americans by 2014.3 To achieve this goal, President George Bush created a new, sub-cabinet level National Health Information Technology Coordinator position at the Department of Health and Human Services to implement health IT infrastructure nationwide. The biggest push targeted towards promoting the adoption of EMR technology came with the passage of the American Recovery and Reinvestment Act (ARRA) 2009 by the U.S. Congress which appropriated $19 billion dollars government assistance to jump start the adoption of EMR technology by physicians, clinics, and hospitals. The healthcare reforms highlighted in the ARRA include an investment of $50 billion in health information technology.4
The U.S. lags behind many industrial nations in adopting EMR technology. A survey study of eleven countries in 2009 revealed that EMR adoption rate was the second lowest in the U.S., only Canada fared worse than the U.S.5 (Chart 1). The Netherlands had the highest EMR technology adoption rate (99%) followed by New Zealand and Norway (97%), United Kingdom (96%), Australia (95%), Italy and Sweden (94%), Germany (72%), France (68%), U.S. (46%), and Canada (37%). Countries like Thailand and India are also leapfrogging the U.S. in adopting sophisticated EHRs technology. Apollo hospital chain in India is believed to have the most advanced EHRs system.6 Why is the U.S. lagging in EMR technology adoption? Several studies have consistently found that initial capital requirements, cost of system maintenance, privacy concerns and resistance from physicians are the major hurdles in EMR technology adoption.7
Seventy-five percent of all physicians in the U.S. practice in small offices with 10 doctors or fewer. This group of office-based physicians exhibit resistance in adopting EMR technology citing high initial costs, system maintenance costs, and uncertain returns from such investments.8 The Obama administration has tried to rally this group of physicians in using extensive EMR technology by providing incentives up to $44,000 per physician spread over multiple years.
Chart 1:
Percent of Physicians Using Electronic Medical Records* in Selected Countries, 2009
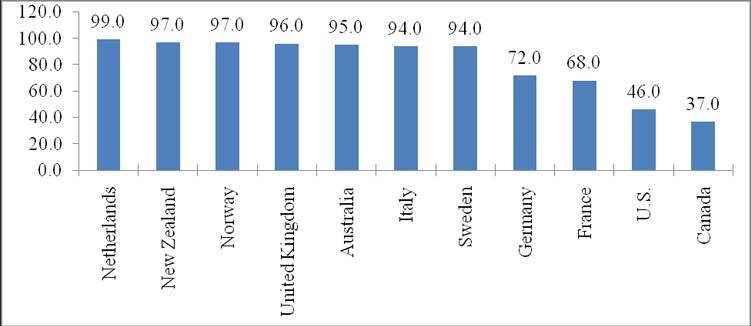
Note:* Not including billing system.
Source: A Survey of Primary Care Physicians in 11 Countries, 2009: Perspectives on Care, Costs, and Experiences, The Commonwealth Fund, web site,
PDF Download
The National Ambulatory Medical Care Survey (NAMCS) conducted annually by the National Center for Health Statistics (NCHS) captures information on use of EMR/EHR by physicians across the U.S. In 2001, only 18 percent of physicians reported to have used any or all EMR/EHR system (not including systems solely for billing). By 2009, nearly 44 percent physicians reported use of any or all EMR/EHR system.9 However, one-fifth of physicians reported using basic EMRs while only 6 percent reported using fully functional EMRs in 200910 (Chart 2). The use of EMRs in U.S. hospitals is also extremely minimal. A recent survey study published in the New England Journal of Medicine revealed that only 1.5 percent of U.S. hospitals had comprehensive electronic record system. Respondents in the survey cited capital requirements and costs of system maintenance as the major barriers in EMR technology implementation. The rate of EMR adoption was found to be higher among large practices than in office-based and smaller practices.11 With the current pace, it will take many years for small practice physician groups, clinics, and hospitals in the U.S. to adopt fully functional EMR system.
Chart 2: Percent of Office-Based Physicians Using Electronic Medical Records/Electronic Health Records (EMRs/EHRs), U.S., 2001-2009
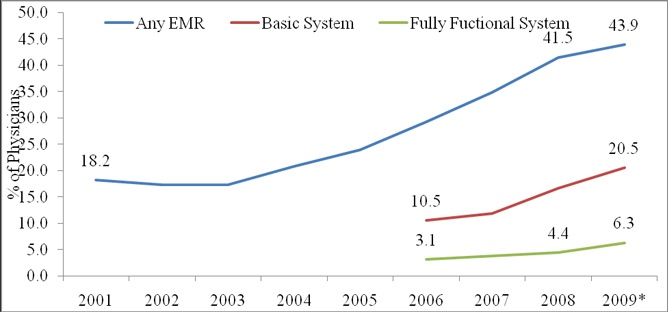
Note:* Preliminary.
Source: CDC/NCHS, National Ambulatory Medical Care Survey, web site,
EMR EHR
Despite these dismal statistics on EMR technology adoption, the current administration’s incentive has brought lots of enthusiasm among office-based physicians, clinics, and hospitals towards using the EMR technology. It is strongly expected that adoption of EMRs will benefit entire healthcare system resulting in the reduction of health care costs, creation of jobs12, and reduction in medical errors, redundant tests and procedures.13 It is also found that the adoption of EMR technology in integrated health care delivery system will improve the efficiency and quality of the care. The Department of Veterans Affairs (VA) and Intermountain Healthcare are the prime examples on this.14 The Congressional Budget Office (CBO) projected $12 billion saving from health IT over 10 years.15 In addition, two studies by RAND Corporation and Center for Information Technology Leadership (CITL) have estimated potential $80 billion in net annual savings with the use of health IT.16 Other studies refute these claims.17 However, physicians in small health care delivery environment argue that costs of EMR adoption and maintenance will exceed the benefits. This is a plausible argument. The vendors of EMR system should take into consideration small practice group’s concerns and tailor EMR software to their needs accordingly. They should find creative ways to deliver EMR system to physicians, clinics, and hospitals at reasonable costs. Ease of use should be a top priority. This will make the transition for EMR users smooth and will prompt others to adopt wider use of the technology. Evidence suggests that a vast majority of physicians who use EHR would not want to return to paper charts if they could.18
The U.S. Department of Health and Human Services (DHHS) is likely assign the Certification Commission for Health Information Technology (CCHIT) with the responsibility of certifying EHR software system or technology. The users of EMR technologies are required to have certified EHR system from the vendors to be eligible for the stimulus incentive. Opponents argue that certification will make the EMR system more expensive for physicians and small practices to implement as EMR vendors will ultimately pass the costs to EMR users. Others argue that certification requirements will also thwart new innovative solutions that are targeted towards specific specialty problems in health care delivery. Dr. David Blumenthal, National Coordinator for Health Information Technology (NCHIT), in a recent New England Journal of Medicine article, opined that many certified EHRs are not user friendly.19 Before purchasing EMR software, users are advised to create a list of features that are important for their practice and ascertain that their chosen EMR system meet those criteria.
Health care practitioners and organizations planning to purchase EMR technology should be cautious about the sales pitch from vendors and consultants. There are hundreds of EMR providers in the U.S.20 Buyers should be wary of vendors offering “one size fits all” EMR products. Ideally an EMR would be designed with active input from health care practitioners as they best know the practice workflow and understand how to make the system more efficient. Before making a purchase, one should thoroughly review the costs of EMR technology adoption and system maintenance including the cost of licensing, upgrades, specialty templates, initial technology training, customer support, warranty, and security. Cost of digitizing existing paper records should also be an important criterion. One should take into account how fast and cost effectively vendors can digitize existing paper records.
The U.S. health care industry, despite its sheer size ($2.5 trillion), is one of the laggards in adopting modern information technology. A lot of concerted efforts from heath care practitioners, health care providers, health organizations, developer of healthcare technology, and policy makers are needed to move forward with modernizing health care IT to meet the health care needs of the 21st century. The recent exuberance from practitioners, organization, vendors, and policy makers in adopting EMR technology seems to be promising, but the industry is nowhere near where it should have been at the moment. There are critiques who argue that today’s EMR technologies are designed to improve the efficiency of individual transaction, but not the quality of the health care.21 To achieve quality care, health care information exchange and interoperability are required.22 Information interoperability also should be supplemented by substitutability of the system.23 An ideal EMR system is one where current fragmented system communicate with each other and, as a result, all parties involved get access to better health information. At the next level, after digitizing and making fragmented system communicate with each other, new technologies such as data mining and natural language processing could bring unprecedented amount of health care knowledge and insight. These technologies will help health care practitioners observe and examine patterns or trends in longitudinal patient data and will help them make timely and informed decisions on their patients.24 The European Commission in its recent report highlighted the importance of adopting semantic interoperability (SIOp) of EHR within its member countries.25 While the U.S. lags far behind its European counterparts in SIOp of EHR, the adoption of EMR technologies is the first step to get there.
1 See: Carter, Jerome, MD, Electronic Medical Records: A Guide for Clinicians and Administrators, American College of Physicians, 2001.
2 See: Institute of Medicine (IOM), The Computer-based Record: An Essential Technology for Healthcare, 2nd Edition. Dick, R.S., Steen, E.B., Detmer, D.E., eds., Washington, D.C., National Academy Press, 1997
3 President George W. Bush, Executive Order 13335, accessed from: PDF Download
4 See: American Medical Association, “American Recovery and Reinvestment Act (AARA) of 2009”, accessed from: http://www.ama-assn.org/ama/pub/advocacy/current-topics-advocacy/hr1-stimulus-summary.shtml
5 See: Cathy Schoen, Robin Osborn, Michelle M. Doty, David Squires, Jordon Peugh and Sandra Applebaum,
“A Survey Of Primary Care Physicians In Eleven Countries, 2009: Perspectives On Care, Costs, And Experiences”, Commonwealth Fund, web site, PDF Schoen 2009
6 See: “Hit or Miss”, The Economist, v392 n8627 pHC4(3), April 18, 2009.
7 See: (a). DesRoches C, Campbell E, Rao S, et. Al., “Electronic health records in ambulatory care- a national survey of physician”, The New England Journal of Medicine, 2008; 359(1):50-60; (b). Nefertiti C. duPont, Danya Koeninger, Joseph D. Guyer, Debbie Travers, “Selecting an Electronic Medical Record System for Small Physician Practices”, The New England Journal of Medicine, September/November 2009, Vol 70. No 5; (c). Jha A, Ferris T, Donelan K, et al., “How common are electronic health records in the United States? A summary of the evidence”, Health Affair (Milwood) 2006;25;w486-w507; (d). Glenn A Loomis, J Scott Ries, Robert M Saywell, Nitesh R. Thakker, “If electronic records are so great, why aren’t family physicians using them?”, The Journal of Family Practice, July 2002, Vol. 51, No. 7, pp. 637-641;(e). Tevi Troy, “5 Myths on Health Care's Electronic Fix-It”, Washington Post, April 26, 2009; (f). Miller, Robert H., and Ida Sim. 2004. “Physicians’ Use of Electronic Medical Records: Barriers and Solutions.” Health Affairs, vol. 23, no. 2 (March–April), pp. 116–126.
8 See: Jha A, op, cit.
9 See: Chun-Ju Hsiao, Paul C. Beaty, Esther S. Hing, David A. Woodwell, Elizabeth A. Rechtsteiner, and Jane E. Sisk, Electronic Medical Records/Electronic Health Records Use by Office Based Physicians: United States, 2008 and Preliminary 2009, Center for Disease Control, National Center for Health Statistics, December 2009.
10 The questionnaire asked physicians to identify multiple functionalities of EMR/EHR systems. According to the CDC report, basic EMR system include functionalities such as demographic information, patient problem lists, clinical notes, orders for prescriptions, and viewing laboratory results and imaging. Fully functional system include basic system and others such as medical history and follow-up, orders for tests, prescription and test orders sent electronically, warnings of drug interactions or contraindication, highlighting of out-of-range test levels, and reminders for guideline-based interventions.
11 See: Ashis K. Jha, Catherine M. DesRoches, Eric G. Campbell, Karen Donelan, Sowmya R. Rao, Timothy G. Ferris, Alexandra Shields, Sara Rosenbaum, and David Blumenthal, “Use of Electronic Health Records in U.S. Hospitals”, The New England Journal of Medicine, March 2009, 460:16, pp 1628-38.
12 The U.S. Bureau of Labor Statistics projects above average growth of 20 percent over the 2008-2018 period in medical records and health information tchnicians occupations, for more information, see: Bureau of Labor Statistics, U.S. Department of Labor, Occupational Outlook Handbook, 2010-11 Edition, Medical Records and Health Information Technicians, on the Internet at http://www.bls.gov/oco/ocos103.htm (visited February 09, 2010).
13 See: (a). Bates, David W., and others. 2003. “Ten Commandments for Effective Clinical Decision Support: Making the Practice of Evidence-Based Medicine a Reality.” Journal of the American Medical Informatics Association, vol. 10, no. 6 (November–December), pp. 523–530; (b). Kaushal, Rainu, and others. 2006. “Return on Investment for a Computerized Physician Order Entry System.” Journal of the American Medical Informatics Association, vol. 13, no. 3 (May–June), pp. 261–266.
14 Evans, Dwight C., Paul W. Nichol, and Jonathan B. Perlin. 2006. “Effect of the Implementation of an Enterprise-Wide Electronic Health Record on Productivity in the Veterans Health Administration.” Health Economics.
15 See: Evidence on the Costs and Benefits of Health Information Technology, A Congressional Budget Office (CBO) Paper, The Congress of the United States, May 2008.
16 See: Kateryna Fonkych and Roger Taylor, The State and Pattern of HEALTH Information Technology Adoption, RAND Corporation, 2005.
17 See: (a). Stephen T. Parente and Jeffrey S. McCullough, “Health Information Technology And Patient Safety: Evidence From Panel Data”, Health Affairs, 28, no. 2 (2009): 357-360; (b). David U. Himmelstein and Steffie Woolhandler, “Hope And Hype: Predicting The Impact Of Electronic Medical Records”, Health Affairs, September/October 2005, Volume 24, Number 5.
18 See: Robert L. Edsall and Kenneth G. Adler, “User Satisfaction With EHRs: Report of a Survey of 422 Family Physicians”, American Academy of Family Physicians, 2008, web site, http://www.aafp.org/fpm/2008/0200/p25.pdf
19 See: David Blumenthal, “Stimulating the Adoption of Health Information Technology”, The New England Journal of Medicine, 360;15 (2009), pp. 1477-1479.
20 EMR Experts, Inc., (www.emrexperts.com) lists 210 EMR vendors in their web site in 2009.
21 See: Leonard W. D’Avolio, “Electronic Medical Records at a Crossroads: Impetus for Change or Missed Opportunity”, The Journal of the American Medical Association, 2009;302(10):1109-1111.
22 See: David J. Brailer, “Interoperability: The Key To The Future Health Care System”, Health Affairs, 19 January, 2005, web site.
23 See: Kenneth D. Mandl and Isaac S. Kohane, “No Small Change for the Health Information Economy”, The New England Journal of Medicine, 2009, 360:13, pp 1278-1281.
24 See: Steve Lohar, “Health Care Industry Moves Slowly Onto the Internet”, New York Times, April 5, 2009.
25 See: Stroetmann et.al., “Semantic Interoperability for Better Health and Safer Healthcare”, European Commission, January 2009, accessed web site, 2009 Semantic Health Report
About the Authors
Ishwar Khatiwada
Ishwar Khatiwada is a research economist at the Center for Labor Market Studies, Northeastern University. He has extensive experience in economic analysis, including U.S. labor market and industry analysis. Mr. Khatiwada’s work has been featured in many books, research monographs, and national and international popular media. His research work was recently featured in:
- Time CNN (http://curiouscapitalist.blogs.time.com/2010/02/10/rich-people-still-have-jobs-poor-people-dont/)
- Reuters (http://blogs.reuters.com/felix-salmon/2010/02/11/the-massive-cost-of-underemployment/ )
- New York Times (http://www.nytimes.com/2010/02/09/opinion/09herbert.html?scp=2&sq=bob%20herbert&st=cse )
- Wall Street Journal (http://blogs.wsj.com/wealth/2010/02/12/high-unemployment-not-for-the-affluent/)
- Huffington Post (http://www.huffingtonpost.com/2010/02/10/no-labor-market-recession_n_456797.html )
- Boston Herald (http://bostonherald.com/business/general/view.bg?articleid=1230768&position=1 )
- Daily Finance (http://www.dailyfinance.com/story/recession-hammers-low-wage-workers-but-glances-off-the-affluent/19354990/ )
- Challenge Magazine (http://mesharpe.metapress.com/app/home/contribution.asp?referrer=parent&backto=issue,6,9;journal,2,55;linkingpublicationresults,1:106043,1)
- Community and Banking (http://www.bos.frb.org/commdev/c&b/2010/winter/Andrew_Sum_Black_Males.pdf )
- The National Business Review (http://www.nbr.co.nz/article/who-knew-poor-were-underemployed-118438)
- The Economist (http://www.economist.com/blogs/democracyinamerica/2010/02/tax_breaks_hiring_workers)
- National Public Radio (NPR) (http://www.onpointradio.org/2010/02/unemployment-and-inequality)
- St. Louise Dispatch (http://interact.stltoday.com/blogzone/stl-jobwatch/recession/2010/02/report-recession-slammed-low-income-households-the-hardest/)